That's kind of naive. One can make data and statistics look like all kinds of things. Seriously?You skipped that the first source which is the CDC.
The great thing about data is that it is neutral and based on math and science, not opinion.

You are using an out of date browser. It may not display this or other websites correctly.
You should upgrade or use an alternative browser.
You should upgrade or use an alternative browser.
Coronavirus - Excellent Data-Based Analysis
- Thread starter sswartz
- Start date
COVID mortality rate 2 to 3.4% No wait..1.4% Today it is .66%, I hope it keeps going down. But the real numbers have yet to be determined.
"Science doesnt have a political philosphy" Only the people that write about it do. I guess we will see when this whole thing shakes out. I think we know where each other stands.
"Science doesnt have a political philosphy" Only the people that write about it do. I guess we will see when this whole thing shakes out. I think we know where each other stands.
You are on a data-based analysis thread. If you believe that data is being fabricated then start a thread to discuss that. This is a thread about looking at the data, not speculating and trying to bring political views into it.
From Worldometer

There are 674,829 cases in the USA of which 34,475 have died. Only the cases with actual outcomes can be represented by the data so at this point the death rate is 38%.
Considering all the cases active or not active in the USA, 5.1% have died.

From Worldometer
There are 674,829 cases in the USA of which 34,475 have died. Only the cases with actual outcomes can be represented by the data so at this point the death rate is 38%.
Considering all the cases active or not active in the USA, 5.1% have died.
You’re right Jared, there is uncertainty around the mortality rate that directly affects the accuracy of the model. In fact any predictive model contains errors and uncertainties. Even the IHME models that have proved to be very accurate so far, have significant error bars around their projections i.e. refer to the shaded areas around their best estimate lines.
So I would make 2 observations;
You mention a wide range of mortality rates; 0.66 to 3.4%. I have used a median value of 1%. This was based on reviewing several analytical articles and was the value proposed by Dr Fauci director of the National Institute of Allergy and Infectious Diseases . However, I believe there is some evidence that it could be as high as 2% when applied specifically to the US. All higher values quoted were in situations where the health care system was being overwhelmed and testing had collapsed to tests only for the more serious cases. There is considerable evidence to support this.
The other end of the scale (0.65%) was from S. Korea and Germany. I am hoping this will turn out to be the case but don’t think it will. My reasoning is that both those countries instituted aggressive testing and tracing from the get-go. As a result, the virus never became widespread in their populations and from what I have read did not spread significantly to care homes or other areas with vulnerable populations.
It’s a simple task to use a different MR in the model to see its effect on the projected infection (to the end of April). As mentioned previously, with 1% MR the model projects a level of infection of roughly 7 million (about 2 % of the population) with 88% of cases undetected. This is close to the 86% that the article referred to has estimated based on their analysis of the statistics (which you may or may not choose to consider).
With a 2% MR, the level of infection would be about 3.5million (about 1%) with about 76% of cases undetected, and with a 0.7% MR it would be about 10 million (about 3% of the pop) with about 92% of cases undetected.
With this level of uncertainty acknowledged in the model, the next step is to go back and review the basic findings as stated in my post 72. I don’t believe it changes my conclusions but would be interested to hear your views.
So I would make 2 observations;
- just because there are uncertainties involved doesn’t mean you shouldn’t attempt to evaluate the problem using best information possible
- models have the useful function of being able to vary parameters to determine their effect on the output (sensitivity analysis)
You mention a wide range of mortality rates; 0.66 to 3.4%. I have used a median value of 1%. This was based on reviewing several analytical articles and was the value proposed by Dr Fauci director of the National Institute of Allergy and Infectious Diseases . However, I believe there is some evidence that it could be as high as 2% when applied specifically to the US. All higher values quoted were in situations where the health care system was being overwhelmed and testing had collapsed to tests only for the more serious cases. There is considerable evidence to support this.
The other end of the scale (0.65%) was from S. Korea and Germany. I am hoping this will turn out to be the case but don’t think it will. My reasoning is that both those countries instituted aggressive testing and tracing from the get-go. As a result, the virus never became widespread in their populations and from what I have read did not spread significantly to care homes or other areas with vulnerable populations.
It’s a simple task to use a different MR in the model to see its effect on the projected infection (to the end of April). As mentioned previously, with 1% MR the model projects a level of infection of roughly 7 million (about 2 % of the population) with 88% of cases undetected. This is close to the 86% that the article referred to has estimated based on their analysis of the statistics (which you may or may not choose to consider).
With a 2% MR, the level of infection would be about 3.5million (about 1%) with about 76% of cases undetected, and with a 0.7% MR it would be about 10 million (about 3% of the pop) with about 92% of cases undetected.
With this level of uncertainty acknowledged in the model, the next step is to go back and review the basic findings as stated in my post 72. I don’t believe it changes my conclusions but would be interested to hear your views.

Coronavirus State-By-State Projections: When Will Each State Peak?
Wondering how bad the coronavirus crisis is going to get where you live? New modeling offers state-by-state projections.
 www.npr.org
www.npr.org
I don't recall bringing in any political views. I think you might be projecting. The "Scientists" have a mortality rate close to 1% percent at this point. It doesn't take that much of an objective thinker to realize the data you are presenting is skewed to the worst-case scenario. Those who were sick enough to get tested and no doubt the cases that found themselves in the hospital. You can continue to choose to look at the numbers that support your opinion that this is a deadly virus. Unless you are of advanced age or have a preexisting condition you will likely be unscathed by this virus.You are on a data-based analysis thread. If you believe that data is being fabricated then start a thread to discuss that. This is a thread about looking at the data, not speculating and trying to bring political views into it.
From Worldometer
View attachment 105754
There are 674,829 cases in the USA of which 34,475 have died. Only the cases with actual outcomes can be represented by the data so at this point the death rate is 38%.
Considering all the cases active or not active in the USA, 5.1% have died.
View attachment 105753
I don't recall bringing in any political views. I think you might be projecting. The "Scientists" have a mortality rate close to 1% percent at this point. It doesn't take that much of an objective thinker to realize the data you are presenting is skewed to the worst-case scenario. Those who were sick enough to get tested and no doubt the cases that found themselves in the hospital. You can continue to choose to look at the numbers that support your opinion that this is a deadly virus. Unless you are of advanced age or have a preexisting condition you will likely be unscathed by this virus.
There are a lot of deceased young people with no preexisting conditions that would disagree with you .If they could.
Really? How many? Did you review their medical history and death certification? I did read a news report of a 45-year-old man who died of "coronavirus" complications. I also know that person was HIV positive, overweight and smoked weed. My point is of course that unless you are intimately familiar with someone's medical history and the lifestyle it is difficult if not impossible to know what preexisting conditions were a factor. We just don't have access to that info. Unless you are a medical doctor and speaking from experience then I stand corrected. Lower respiratory illness already was in the top 4 of killers in this country before COVID came along. I am still trying to remain fact-based.There are a lot of deceased young people with no preexisting conditions that would disagree with you .If they could.
Jared,Really? How many? Did you review their medical history and death certification? I did read a news report of a 45-year-old man who died of "coronavirus" complications. I also know that person was HIV positive, overweight and smoked weed. My point is of course that unless you are intimately familiar with someone's medical history and the lifestyle it is difficult if not impossible to know what preexisting conditions were a factor. We just don't have access to that info. Unless you are a medical doctor and speaking from experience then I stand corrected. Lower respiratory illness already was in the top 4 of killers in this country before COVID came along. I am still trying to remain fact-based.
It is difficult to write this without sounding sanctimonious, or look as though I am singling you out, as unfortunately you are far from the only one who holds the same view. In the past few hours while you were trying to remain fact-based, without it would seem in my experience and opinion to actually have all the facts to hand, if you believe this virus is resticted to killing people with underlying health conditions. One of our 2 children who both work on the front line for the ambulance service, was out in the Northwest of the UK trying unsuccessfully to save lives.
Both are children are really concerned especially as one of them has an underlying health condition which could have serious consequences if they catch the virus. They have never been worried before, or at the beginning of this pandemic. It's the same with many doctors, they are equally concerned. If we say we value and applaud these people as we do in the UK every Thursday at 8pm, we, also need to listen to them, and in my opinion if they are worried, we need to worry.
I will leave the last comment to our son who sent me a message this morning after finishing his shift and has since rung to insist he will do our shopping for us and we are not to go out.
“Just be careful I’ve basically done a full block of watching people fighting for breath and dying in front of us and no matter what we do nothing works I’ve never felt so useless when the family are begging you to do something”
Nick
No problem singling me out. I asked for it. The world is lucky to have people like your son. Under "normal" circumstances that is a tough job. They are rarely in contact with someone who is not in dire need. Unfortunately, they have the highest risk of exposure having to be in close contact with sick folks on a regular basis. I have been fortunate (or unfortunate) to be on the receiving end of some fantastic medical care recently. These people amaze me.Jared,
It is difficult to write this without sounding sanctimonious, or look as though I am singling you out, as unfortunately you are far from the only one who holds the same view. In the past few hours while you were trying to remain fact-based, without it would seem in my experience and opinion to actually have all the facts to hand, if you believe this virus is resticted to killing people with underlying health conditions. One of our 2 children who both work on the front line for the ambulance service, was out in the Northwest of the UK trying unsuccessfully to save lives.
Both are children are really concerned especially as one of them has an underlying health condition which could have serious consequences if they catch the virus. They have never been worried before, or at the beginning of this pandemic. It's the same with many doctors, they are equally concerned. If we say we value and applaud these people as we do in the UK every Thursday at 8pm, we, also need to listen to them, and in my opinion if they are worried, we need to worry.
I will leave the last comment to our son who sent me a message this morning after finishing his shift and has since rung to insist he will do our shopping for us and we are not to go out.
“Just be careful I’ve basically done a full block of watching people fighting for breath and dying in front of us and no matter what we do nothing works I’ve never felt so useless when the family are begging you to do something”
Nick
I didn't write the virus was "restricted" to killing people with underlying conditions. I did say the vast majority (largely) that perish are of advanced age or have preexisting conditions. In reference to my facts or lack of. At this point, .003% of the world population has been killed by COVID which is about how many people die worldwide per day for some perspective. And we seem to be on the other side of it. If anything we are better at testing and treating it.
I didn't write the virus was "restricted" to killing people with underlying conditions. I did say the vast majority (largely) that perish are of advanced age or have preexisting conditions. In reference to my facts or lack of. At this point, .003% of the world population has been killed by COVID which is about how many people die worldwide per day for some perspective. And we seem to be on the other side of it. If anything we are better at testing and treating it.
I guess it can also depend on what you consider advanced age, I am in my late 50’s and don’t consider myself to be old, but according to our sons experience I am at prime age for not surviving it.
As I was trying to point out the medical profession are well used to the normal number of people dying, they deal with it every day. I have yet to see any doctor that is not really concerned by the current situation.
I hope you can see this video and I hope you watch it all the way through especially when he is talking about the age of victims
indeed they should. And that is a whole different topic. Education.they really should teach more science in schools...................
Nothing personal,but I believe that down playing this disease is killing people. I also have someone on the frontlines of this pandemic and it is just hammering their morale into the ground. They risk their lives EVERYDAY only to here "its just another flu etc". People take it lightly get infected and the healthcare workers have to risk THIER lives treating them. Otherwise healthy Drs and nurses as well as respiratory therapists and other health care workers are dying from covid 19. I may be wrong have not heard of Drs or Nurses dying from treating the flu.
I guess it can also depend on what you consider advanced age, I am in my late 50’s and don’t consider myself to be old, but according to our sons experience I am at prime age for not surviving it.
As I was trying to point out the medical profession are well used to the normal number of people dying, they deal with it every day. I have yet to see any doctor that is not really concerned by the current situation.
I hope you can see this video and I hope you watch it all the way through especially when he is talking about the age of victims
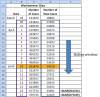
As far as age and underlying conditions both being factors this data seems to support my unpopular opinion. (I called it my opinion) This is data from NYC. You could argue the relevance outside of NYC of course. So according to this data 59 out of 1581 age 45-64 did not have underlying cond. as a contributor to death.
AGE | Number of Deaths | Share of deaths | With underlying conditions | Without underlying conditions | Unknown if with underlying cond. | Share of deaths of unknown + w/o cond. |
0 - 17 years old | 3 | 0.04% | 3 | 0 | 0 | 0% |
18 - 44 years old | 309 | 4.5% | 244 | 25 | 40 | 1.0% |
45 - 64 years old | 1,581 | 23.1% | 1,343 | 59 | 179 | 3.5% |
65 - 74 years old | 1,683 | 24.6% | 1,272 | 26 | 385 | 6.0% |
75+ years old | 3,263 | 47.7% | 2,289 | 27 | 947 | 14.2% |
TOTAL | 6,839 | 100% | 5,151 | 137 | 1,551 | 24.68% |
Abstract
Background: Little is known about factors associated with hospitalization and critical illness in Covid-19 positive patients. Methods: We conducted a cross-sectional analysis of all patients with laboratory-confirmed Covid-19 treated at a single academic health system in New York City between March 1, 2020 and April 2, 2020, with follow up through April 7, 2020. Primary outcomes were hospitalization and critical illness (intensive care, mechanical ventilation, hospice and/or death). We conducted multivariable logistic regression to identify risk factors for adverse outcomes, and maximum information gain decision tree classifications to identify key splitters. Results: Among 4,103 Covid-19 patients, 1,999 (48.7%) were hospitalized, of whom 981/1,999 (49.1%) have been discharged home, and 292/1,999 (14.6%) have died or were discharged to hospice. Of 445 patients requiring mechanical ventilation, 162/445 (36.4%) have died. Strongest hospitalization risks were age ≥75 years (OR 66.8, 95% CI, 44.7-102.6), age 65-74 (OR 10.9, 95% CI, 8.35-14.34), BMI>40 (OR 6.2, 95% CI, 4.2-9.3), and heart failure (OR 4.3 95% CI, 1.9-11.2). Strongest critical illness risks were admission oxygen saturation <88% (OR 6.99, 95% CI 4.5-11.0), d-dimer>2500 (OR 6.9, 95% CI, 3.2-15.2), ferritin >2500 (OR 6.9, 95% CI, 3.2-15.2), and C-reactive protein (CRP) >200 (OR 5.78, 95% CI, 2.6-13.8). In the decision tree for admission, the most important features were age >65 and obesity; for critical illness, the most important was SpO2<88, followed by procalcitonin >0.5, troponin <0.1 (protective), age >64 and CRP>200. Conclusions: Age and comorbidities are powerful predictors of hospitalization; however, admission oxygen impairment and markers of inflammation are most strongly associated with critical illness.
Background: Little is known about factors associated with hospitalization and critical illness in Covid-19 positive patients. Methods: We conducted a cross-sectional analysis of all patients with laboratory-confirmed Covid-19 treated at a single academic health system in New York City between March 1, 2020 and April 2, 2020, with follow up through April 7, 2020. Primary outcomes were hospitalization and critical illness (intensive care, mechanical ventilation, hospice and/or death). We conducted multivariable logistic regression to identify risk factors for adverse outcomes, and maximum information gain decision tree classifications to identify key splitters. Results: Among 4,103 Covid-19 patients, 1,999 (48.7%) were hospitalized, of whom 981/1,999 (49.1%) have been discharged home, and 292/1,999 (14.6%) have died or were discharged to hospice. Of 445 patients requiring mechanical ventilation, 162/445 (36.4%) have died. Strongest hospitalization risks were age ≥75 years (OR 66.8, 95% CI, 44.7-102.6), age 65-74 (OR 10.9, 95% CI, 8.35-14.34), BMI>40 (OR 6.2, 95% CI, 4.2-9.3), and heart failure (OR 4.3 95% CI, 1.9-11.2). Strongest critical illness risks were admission oxygen saturation <88% (OR 6.99, 95% CI 4.5-11.0), d-dimer>2500 (OR 6.9, 95% CI, 3.2-15.2), ferritin >2500 (OR 6.9, 95% CI, 3.2-15.2), and C-reactive protein (CRP) >200 (OR 5.78, 95% CI, 2.6-13.8). In the decision tree for admission, the most important features were age >65 and obesity; for critical illness, the most important was SpO2<88, followed by procalcitonin >0.5, troponin <0.1 (protective), age >64 and CRP>200. Conclusions: Age and comorbidities are powerful predictors of hospitalization; however, admission oxygen impairment and markers of inflammation are most strongly associated with critical illness.
As far as age and underlying conditions both being factors this data seems to support my unpopular opinion. (I called it my opinion) This is data from NYC. You could argue the relevance outside of NYC of course. So according to this data 59 out of 1581 age 45-64 did not have underlying cond. as a contributor to death.
[1] Underlying illnesses include Diabetes, Lung Disease, Cancer, Immunodeficiency, Heart Disease, Hypertension, Asthma, Kidney Disease, and GI/Liver Disease. [source]
Number of Deaths Share of deaths With underlying conditions Without underlying conditions Unknown if with underlying cond. Share of deaths
of unknown + w/o cond.
G-I-G-O
--------
Preface: Before my retirement in 2015, I was a Systems Architect Technology Manager for one of the largest financial institutions in the free world. My last "gig" was to lead teams that designed, implemented and managed one of the largest Enterprise Wide Active Data Warehouses.
The most important Tenet of Data Warehousing and Analytics is that of "One Version of the Truth - OVT".
IE - Data must be managed consistently, be corroborated and timely.
In short - OVT means that all reporting agencies must adhere to the exact same rules where data purity is of preeminent importance.
If you don't have data purity, analytics mean nothing.
Why?
G-I-G-O
Garbage In Garbage Out.
----
Until all the countries reporting adhere to the same set of rules - those country's data is not only suspect, but worthless.
--------
Preface: Before my retirement in 2015, I was a Systems Architect Technology Manager for one of the largest financial institutions in the free world. My last "gig" was to lead teams that designed, implemented and managed one of the largest Enterprise Wide Active Data Warehouses.
The most important Tenet of Data Warehousing and Analytics is that of "One Version of the Truth - OVT".
IE - Data must be managed consistently, be corroborated and timely.
In short - OVT means that all reporting agencies must adhere to the exact same rules where data purity is of preeminent importance.
If you don't have data purity, analytics mean nothing.
Why?
G-I-G-O
Garbage In Garbage Out.
----
Until all the countries reporting adhere to the same set of rules - those country's data is not only suspect, but worthless.
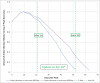
Update: The latest IHME projection has risen for the first time in the last 3 updates. This is likely a result of the high level of new cases being reported since the declared peak (April 10th). In the 7 days since the peak of 34.6k cases being reported, on 4 of the days there have been over 30k new cases and no definite downward trend has yet appeared. I have updated up relative infection curve since the peak (10th) accordingly. The projected relative infection is higher than the previous estimate (see post 64). As mentioned before, it's based on a sliding window sum of 18 days (the assumed amount of time between test and patient becoming virus free). I've included an example based on the latest daily info. The reason for the currently continuing increase is that new cases are being added faster than cases are being dropped from the back edge of the window.
Attachments
Similar threads
- Replies
- 18
- Views
- 7K
- Replies
- 24
- Views
- 4K
- Replies
- 18
- Views
- 4K
- Replies
- 3
- Views
- 1K